
Managed Behavioral Health: Measurement
Previous attempts to reduce the costs of behavioral health services have failed and Healthplan profits have increased. Increases in psychotherapy reimbursement have been little that psychotherapy, based on cost of living and cost of practice, should be 40% to 60% greater than they currently are. Part of the reason for the failures of attempts at reducing cost has been a lack of appropriate and accountable incentives and reimbursements for care providers. Cost control efforts like utilization review provide no incremental improvement or focus on quality of care. Healthplans have been interested in Value-Based Contracting for behavioral health services but have failed for two reason. The technology has been designed to primarily to serve Healthplans not providers and consumers. Healthplans want providers to use outcome informed care methods, assert they have right to provider and patient data, and support technologies that give them direct visible access to patient and provider data. This data has tremendous financial value and Healthplans want to capitalize on the effort of providers who are willing to gather the data and give it to Healthplans.
For more information see:
Value-Based Contracting For Psychotherapy: The New Normal?
https://www.amha-or.com/value-based-contracting-for-psychotherapyDo Not Give Healthplans Your Patient’s Assessment and Outcomes Data
https://www.amha-or.com/do-not-give-healthplansSurvive and Thrive In Private Mental Health Practice
https://www.amha-or.com/survive-thrive-materials
What are managed behavioral health companies telling Healthplans in Oregon?
Separating the intake assessment process from psychotherapy results in higher drop out, lower and longer treatment response, and higher costs.

As many as 85% of therapists believe they help far more people than they do. Approximately 10% of adults deteriorate while in psychotherapy. Between 14 and 25% of children are worse off following psychotherapy. Serious deterioration is recognized in only one-third of psychotherapy cases.
Multiple, sophisticated, real world studies find no difference in outcomes among people treated with different psychotherapy approaches. Factors related to the psychotherapy relationship (i.e., empathy, collaboration, affirmation, genuineness) have a far greater impact on outcome (7:1) than treatment approach, adherence to treatment protocol, or rated competence.

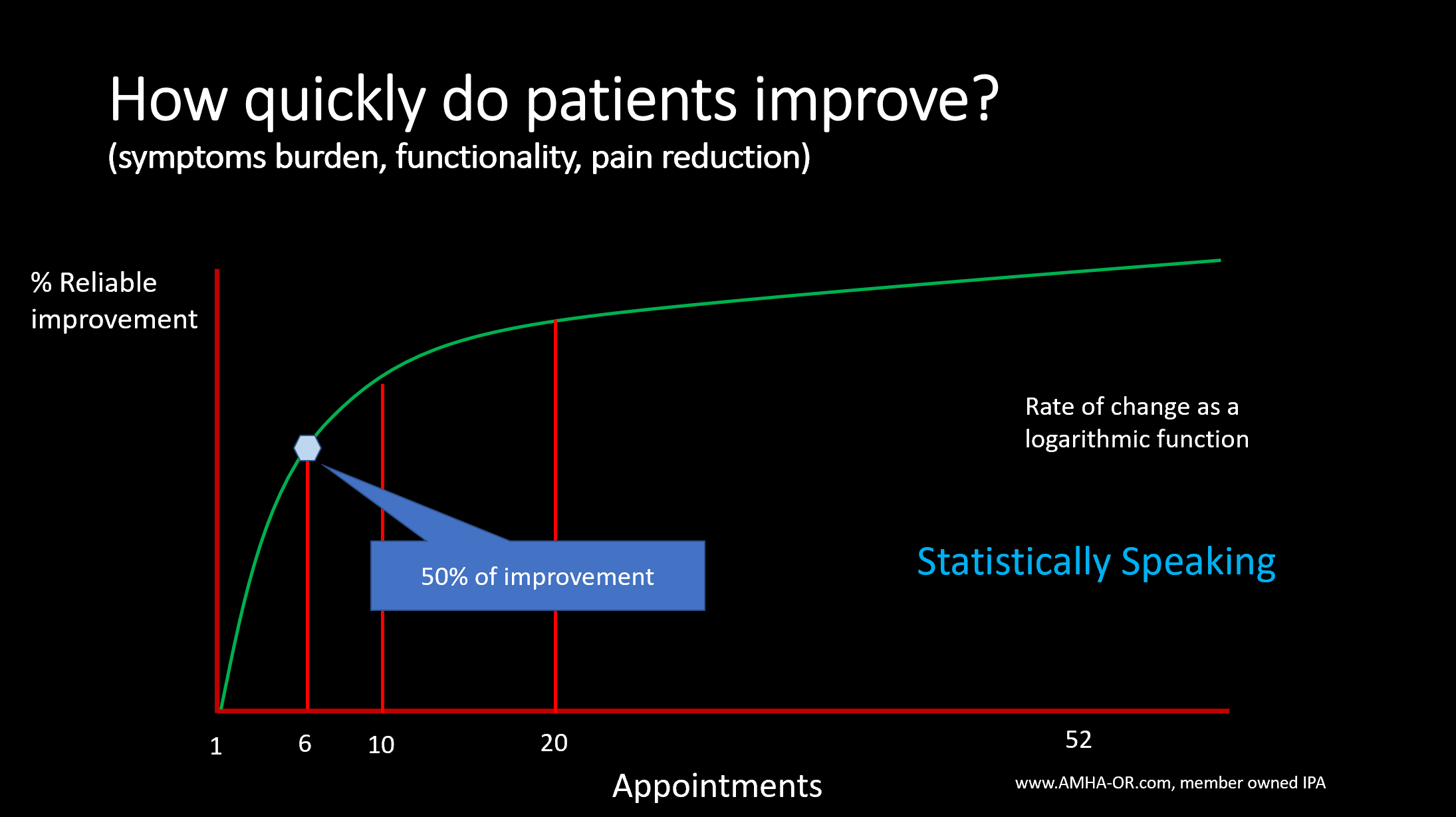
Rapid and dramatic change occurs in as many as 40% of clients in the first 5 appointments and is maintained at two year follow up. There is 90% chance of failure if there is no change between the 2nd and 8th psychotherapy visits. As many as 25% of people remain in treatment while experiencing no measurable benefit.
Around 16% of practitioners achieve outcomes significantly below average. Less effective psychotherapists rate empathic understanding more highly as a professional/personal attribute than more effective psychotherapists. If the clients of the least effective psychotherapists were assigned to an average psychotherapist, an additional 15% of clients would achieve clinical recovery.
Around 16% of psychotherapists consistently achieve outcomes significantly above average. Professional self-doubt and an “error-centric attitude” are associated with better outcomes. More effective psychotherapists rate resilience and mindfulness more highly as a professional/personal attribute.

When psychotherapists receive feedback that clients are deteriorating, they: discuss it with clients about 60% of the time. make efforts to assist with other resources about 27% of the time. adjust therapeutic interventions 30% of the time. vary intensity or dose of services 9% of the time. consult with others (supervision, education, etc.) 7% of the time.

In this example the patient improves quickly in 9 session, relapses and then begin to improve again by session 20. This illustrates that the mathematical model used to predict outcome can predict much different results.
Therapist attitudes toward soliciting and using feedback vary and influence results. Therapists who value feedback achieve better outcomes.
Professional self-doubt and an “error-centric attitude” are associated with better outcomes. When asked, 92% of clients say they like the use of outcome measures in care.
Whose Services are Healthplans Using to Measure and Manage Psychotherapy Services?
There are at least 8 Software companies that have contracts or are seeking contracts to provide therapy outcome measurement in Oregon.
Regional Healthplans each serve approximately 250,000 to several million commercial, Medicaid and Medicare members.
The Healthplans are seeking to “partner” and “provide” infrastructure to “support” and/or “compel” their contracted providers to adopt outcome-informed care (OIC) for behavioral health treatment.
All Healthplans assert that they offer best-in-class behavioral health services to their members.
Healthplans also assert that outcome-informed care (OIC) is a key element in ensuring members receive effective treatment.
The COVID pandemic created nearly a 30% increase in demand for services.
Healthplans are already contracting and identifying the relative strengths and viability of vendors supporting OIC with the aim of contracting with one or more vendors to provide OIC infrastructure to their contracted BH providers.



Effective Date: January 1, 2020
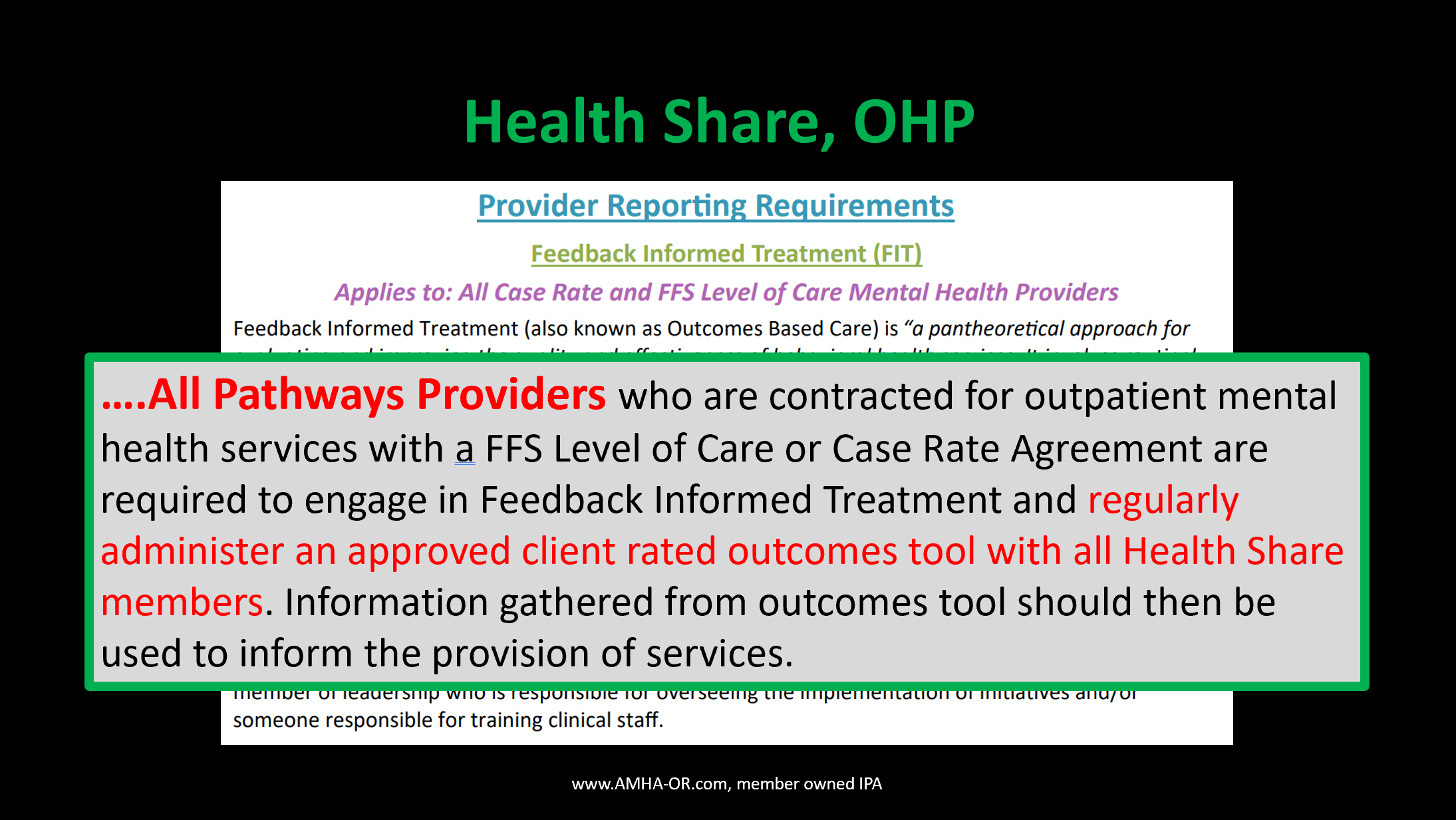
“The following information on outcomes applies to all CareOregon providers contracted to offer mental health outpatient services under the case rate or fee for service level of care model.”
“Providers are expected to use a CareOregon-approved outcomes instrument to aid in treatment planning and overall provision of services. All providers contracted January 2018 or later who are contractually required to implement FIT may self-select either the Outcomes Rating Scale (ORS) and Session Rating Scale (SRS) or the ACORN as their outcomes tool.”
“Providers contracted prior to January 2018 may continue to use their previously selected tool.”
“If a provider contracted prior to January 2018 would like to switch their FIT outcomes tool, they may select either the ORS/SRS or the ACORN. It is the expectation that providers will participate in FIT initiatives, utilize the identified outcomes tool with their member population and that they are able to report on their outcomes to CareOregon. Providers who are interested in FIT support, would like information about learning opportunities or have other FIT-related questions should contact a Behavioral Health Outcomes Specialist.”
CareOregon Behavioral Health Metro Area Provider Manual
Page 27
Whatever it is, the way you tell your story online can make all the difference.
PCOMS and MyOutcomes Services Healthplans
According to CareOregon PCOMs and MyOutcomes can be described as follows:
“Feedback-Informed Treatment: Description, Participation and Standards
Feedback-informed treatment (FIT) (also referred to as outcomes-based care, PCOMS, routine outcomes monitoring and measurement-based care) can be described as:
‘A pantheoretical approach for evaluating and improving the quality and effectiveness of behavioral health services. It involves routinely and formally soliciting feedback from consumers regarding the therapeutic alliance and outcome of care and using the resulting information to inform and tailor service delivery” (Bertolino, B., & Miller, S. (eds.) (2011). The ICCE Feedback ‘
Informed Treatment and Training Manuals. Chicago, IL: ICCE Press)
Essentially, this can be distilled down as the process of:
Regularly and formally gathering client feedback about their level of distress (or wellness) and about the alliance between the client and the helper.
Using that data to inform treatment.
Engaging in deliberate practice to help foster professional development.
FIT puts the client’s voice at the center of services as an active participant and driver of the treatment process. Engaging in FIT processes allows clinicians and agencies to capture and tangibly demonstrate the good work they are doing with clients and notifies clinicians when clients are not benefiting so that treatment can be augmented as needed. In short, it is a client- centered process that helps care providers ensure that as many people benefit from services as possible.”
page 27 to 28

ACORN is used nationally and intensively in Oregon by contracted individual providers, programs that have a Oregon Certificate of Approval, and programs funded by Medicaid and the Oregon Health Plan.
ACORN Services for HealthPlans
According to the ACORN collaborative, ACORNS service can be described as follows:
$500 One time set up fee (includes first month's usage costs)
$30/month per active clinician/care coordinator for health plans with over 200 users. $40/month per single user.
Services include:
Unlimited access to the Toolkit for clinicians/care coordinators, staff, care managers and administrators.
Access to our suite of ACORN mobile, online, and paper questionnaires
Access to your organization's data updated in real time*
Access to various reporting features
Staff training and ongoing consultation for Toolkit usage
*Paper forms submitted via fax may require up to 24 hours to populate in Toolkit due to human processing data verification and is priced at an additional $1/form.
Mentor Research Institute published an article titled, “Ethical Informed Consent Motivates Patients to Game Outcome Measures.” The summary of that article is..
Psychotherapy outcomes include symptom burden, social and functional skills, pain experience, physical and social activity, and the patient’s experience.
The bedrock of psychotherapy outcome prediction, established over the past 40 years, is the psychotherapist-patient alliance.
When outcome measures are used by Healthplans to govern psychotherapy treatment decisions, the measures are subverted and are corrupted by patients who have received ethical informed consent.
For more information see:
https://www.mentorresearch.org/informed-consent-motivates-gaming-outcome-measures

Any “purpose” or “requirement” to use a measurement system such as ACORN, PCOMs and MyOutcomes can be legitimately and ethically circumvented when psychotherapists advise Healthplans and patients that alternative method are more useful, reliable and valid for the patients you want to serve effectively.

Providers want to use systems that are not disruptive to service, support their well-being and mental health, that support the therapist-patient alliance, respect minimum necessary requirements, and are useful to the process of care. Systems where the the data is NOT visible to a Healthplan.
